
An Investigation is a deviation report, which has been identified as requiring more in-depth investigation with the involvement of different functional departments.
Root Cause Analysis
- Root Cause Analysis is a problem-solving technique for identifying the basic or cause factor(s) that underlie the occurrence or possible occurrences of an adverse event in a process similar to the diagnosis of disease, with the goal always in the mind of preventing reoccurrence.
- Failure Investigation and Root Cause Analysis shall be carried out when a product does not meet the predetermined specification. Failure is defined as any confirmed out-of-specification (OOS).
- The Root Cause Analysis is aimed at first generating the possible root cause for the problem and then narrowing the focus in to the most probable cause for the problem.
- Whenever a failure is identified in the product the same shall be brought to the notice of Head-QA or designee.
- Failure Investigation and Root Cause Analysis shall be initiated by the concerned department along with QA person. QA head will nominate the team for investigation. The documentation shall be done in failure investigation report.
- Carry out Failure Investigation and Root Cause Analysis using the checklist, but it will not be limited to this checklist and all efforts will be directed to find out the root cause of the failure. Use additional sheets for completing the investigation whenever required.
- The investigation shall be extended to all the batches/products which could have possibly been affected by the failure.
- Quarantine any Component(s) / Bulk products / Finished Products which might have been affected by the failure till the investigation is completed and the decision is made. Initiate this action through QA.
- The investigation may include additional testing of the involved batches/products or components.
Investigation Steps:
- It is the responsibility of the department, where the problem originated, to involve in the investigation in consultation with the QA Department to ensure the adequacy of the investigation.
- The failure Investigation and Root Cause Analysis is aimed at first generating possible root cause for the problem and then narrowing focus into the most probable cause for the problem.
- The Failure Investigation and Root Cause Analysis is done after an event has occurred. It can be used for preventing problems from occurring.
- The investigation team shall perform the investigation using the tools and techniques and investigation checklist.
INVESTIGATION TOOLS
Based on the information available, identify the probable cause for the non-conformance. If the probable cause is not apparent, use the following four techniques but not limited to,
The First Technique to be used for any kind of investigation is “Genchi Genbustu”. The meaning and procedure of this technique is mentioned below.
- “Genchi Genbustu” Technique: Means ‘Go, and see i.e go and see yourself to thoroughly understand the situation.
- Define the problem in detail. Include who, what, when, where and how. Briefly describe why the event is a problem. This should be a statement of facts.
- Ask five “W” and one “H” as mentioned below,
- What?
- Where?
- When?
- Who?
- Why?
- How?
- Observe the problem/situation first hand, personally (not to rely on the report of others).
- Talk to those at the sharp end (counseling).
- Explore the contributing visible and invisible factors.
- Analyze each factor and conclude probability.
The Second Technique i.e. “Brainstorming” may be used to identify the root cause of the problem. The details of Brainstorming are mentioned below.
- Brainstorming: One of the creative problem-solving methods that allow people to come up with suggestions/ideas that could solve the problem or help to identify the root cause of the problem.
- A meeting with the Cross-Functional team may be called to brainstorm on a problem/situation.
- Relevant people shall ask to think and share their views / suggest ideas to overcome the problem.
- All views and suggestions shall analyze to identify the cause of problem.
Third Technique i.e. 5 -WHY technique may be used to identify the cause of the problem as per the steps mentioned below.
- Five –WHY Technique: It is a questions-based technique and shall be used for each possible factor identified for the problem. A question shall ask the right person in the right way at the right time and place.
- Take the problem statement and ask the question “WHY did that happen?”
- For each cause, ask the next “WHY did that happen?”
- Repeat the question until the primary cause is identified.
- The cause, when identified should preclude the recurrence of the identified non-conformance.
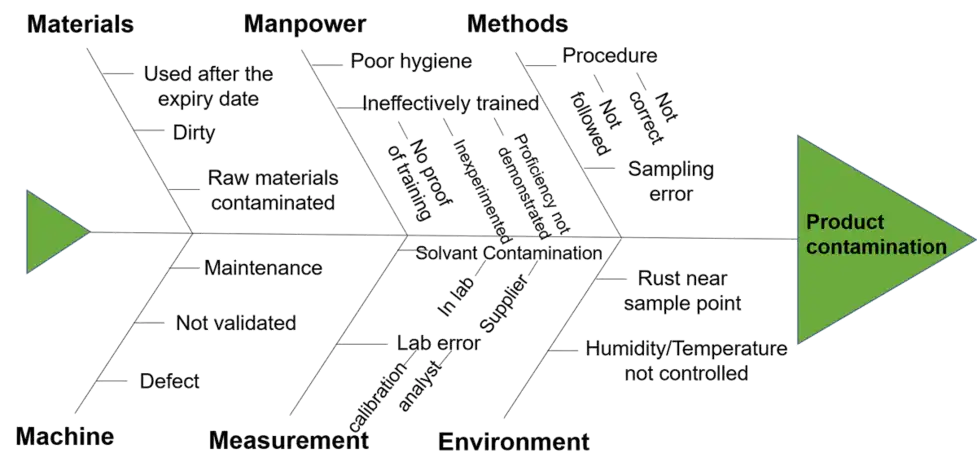
Fourth technique “Six-M Framework” (Ishikawa diagram) using the Fishbone diagram may be used to identify the root cause of the problem. The steps to use “Six M framework” are given below.
Pictorial Presentation of fishbone diagram of Root cause analysis includes,
Head of Fish: Problem of Effect
Bones of the Fish: “Six –M” i.e. Major Causes: Man, Machine/Equipment, Material, Method/Process, Measurement and Environment/Mother Nature etc. More groups can be added, if necessary.
Sub-branches: Sub causes
Define your problem from the following source:
Internal: OOS Reports, Self Inspection, Deviations, Trend analysis, FMEA, Annual Product Quality Review.
External: Market Complaints, Quality / Regulatory Audit Reports etc.
- The Root Cause Analysis team should involve those who are most familiar with the processes and systems and include the participation of the Department Head, Quality Assurance.
- Label each “bone of the fish”. The major categories typically utilized are: Man, Machine/Equipment, Material, Method/Process, Measurement and Environment/Mother Nature.
- The team should identify probable causes, these could be Man, Machine/Equipment, Material, Method/Process, Measurement and Environment/Mother Nature.
FISHBONE DIAGRAM / ISHIKAWA DIAGRAM / CAUSE AND EFFECT DIAGRAM
- Analyze the information and identify the actual or hypothesis. Analysis of data must be objective and logical.
- Determine the extent of the problem. Is this an isolated occurrence limited to one batch or is this a recurring or potentially system-related problem. Evaluate the effects on other processes, products and batches related to a similar problem.
- Propose actions and recommendations for the affected batch(s). Evaluate the following aspect of the batch:
- Quality Aspects such as product safety and integrity, product purity and efficacy, product stability, customer perception and potential complaints.
- Regulatory Aspects such as deviations from product registration commitments.
- Compliance Aspects such as non-compliance of GMPs, or deviations from revalidation / prequalification requirements.
- If an idea fits on more than one branch place it on both, be sure that the causes have a direct, logical relationship to the problem or effect stated at the head of the fish bone. Continue until potential root cause has been identified. A root cause is one that can explain the “Effect” and if removed would eliminate the problem.
1. MATERIAL
- Defective material, Wrong item for use
- Contaminated Material, Wrong specification for use
- Wrong test method (does not evaluate critical material parameters or functionality)
- Outdated material (also see methods), Mix-up in Material
- Inadequate container or storage
- Unacceptable consistency ( in or out of specification)
- Unacceptable supplier/manufacturer performance (quality, delivery)
- Material from Unapproved Sources, Outdated material
- Inadequate Container or Storage, Unacceptable consistency
2. MAN
- Inadequate instruction or training, Human error
- Unauthorized to operate, Unskilled and untrained
- Insufficient number of people, Lack of planning
- Inadequate resource allocation, Inadequate communication
3. MACHINE/EQUIPMENT
- Equipment design inadequate or obsolete for use (capacity, tolerance, speed)
- Incorrect tool selection, Out of calibration
- Facility/room/area design not adequate for use (size, environment, finishes)
- Facilities or equipment not qualified, capability is unknown or not documented
- Facility / room / area fails to maintain specifications(also see design)
- Equipment breakdowns (unpredictable); Capability or reliability unknown
- Equipment not calibrated (also see methods)
- Lack of or inadequate facility maintenance (unscheduled/reactive, routine, preventive, or predictive maintenance)
- Lack of or inadequate equipment maintenance (unscheduled/reactive, routine, preventive, or Predictive)
4. METHOD/PROCESS
- Inadequate design of formulation (stability, functionality)
- Inadequate design of manufacturing process (sequence, timing, complexity)
- Wrong or inadequate equipment (also see equipment)
- Inadequate definition of steps, and critical parameters in batch records
- Process science is not understood (also see people)
- The process is not capable of consistent performance to meet specifications
- The process is not adequately validated; critical parameters are unknown
- Improper process/product test methods and/or specification, No procedure
- Inadequate design for the use (too complicated, too many patches, does not handle expectation, not fail-safe where needed, no feedback or communication loops)
- Inadequate definition or unclear/understandable instructions (critical steps to reproduce the task consistently are not defined in the SOP)
- Ownership (individual) of the tasks and results are not defined
- Accountability for results not accepted (also see people, management)
- Inadequate communication of procedure or results (also see design and management)
- Results of the procedure/process are not measured/trended / communicated
5. MEASUREMENT
- Procedures not followed, Practices are not the same as written procedures,
- Measuring techniques not validated.
6. ENVIRONMENT/MOTHER NATURE
- Weather extremes (temperature, humidity, rain, wind etc.)
- Improper monitoring of temperature
- Humidity conditions and storage conditions during handling/transportation
7. DOCUMENTS
- Forms missing information does not reflect task Format confusing and not user-friendly
- Obsolete or uncontrolled editions
8. NON-ASSIGNABLE CAUSE
- An assignable cause cannot be determined.
- Each alternative shall be analyzed and checked for potential relationships between multiple contributory factors.
- Eliminate alternatives one by one after analysis that could not be the root cause.
- Finally, list the probable cause and identify the exact root cause or causes among them Look for those items that appear in more than one category. These become the “most probable causes”.
- ‘Human error’ can not be the only root cause or primary root cause for any problem. If ‘Human error’ is identified as a cause of the problem then the matter shall be further investigated to identify the root cause to make as an error.
- From those items identified as the “Most Probable Causes,” the team shall reach a consensus using the team’s best collective judgment on listing those items being the “Most Probable Cause”.
- Develop Corrective / Preventive Actions (CAPA) and document them as per SOP for Corrective Action and Preventive Action (CAPA).
- “Corrective and Preventive Action” for the affected batch or batches. Develop preventive actions to avoid recurrence. Corrective and Preventive actions must be monitored to completion.
- Corrective Actions that emerged from the investigation shall be taken with proper change control if required, and follow-up shall be carried out for all the suggested corrective action(s) as per SOP for Corrective Action and Preventive Action.
- The Failure Investigations and Root Cause Analysis Report shall be signed by the QA, Production and any other department involved. The report shall be forwarded to Head-QA for approval.
- Head-QA or designee shall take the final decision, based on the investigation findings.
- The Failure Investigations and Root Cause Analysis Report shall be maintained in the QA documentation cell with all the supporting data. The Designated QA person shall allot the Failure Investigations and Root Cause Analysis Report number.
- A photocopy of the investigation report shall be filed in the Batch production record of the affected batch(es).
- The Head-QA or designee shall ensure that the corrected action has been implemented as per the findings.
- The Failure Investigations and Root Cause Analysis shall be completed within 30 working days from the initiating date. If the investigation could not be completed within the stipulated time, mention justification and tentative time for the completion of the investigation, and should be addressed through SOP for “Period Extension for Document Closing”.
.webp)



.webp)






{kind=link}
0 Comments